Heterotopic pregnancy, defined as the coexistence of intrauterine and extrauterine gestations, is a rare but potentially life-threatening condition in spontaneous conceptions. Ovarian ectopic pregnancy is itself an uncommon form of ectopic pregnancy, making ovarian heterotopic pregnancy exceptionally rare. This is a case of spontaneous heterotopic pregnancy in a woman with a history of multiple prior medical abortions, presenting with a failed intrauterine pregnancy and persistent right ovarian ectopic gestation. Early diagnosis through serial ultrasonography and prompt surgical intervention resulted in a favourable maternal outcome.

Case Report
Persistence of a Right Ovarian Ectopic Pregnancy Following Failure of the Intrauterine Component of a Spontaneous Heterotopic Pregnancy: A Rare Case Report
Dayna Shroff* 
Abstract
Keywords: Heterotopic pregnancy, Ovarian ectopic pregnancy, Retained products of conception, Spontaneous conception
Introduction
Heterotopic pregnancy refers to the simultaneous presence of an intrauterine and an ectopic pregnancy. The incidence in spontaneous conception is estimated to be approximately 1 in 30,000 pregnancies but is increasing due to the widespread use of assisted reproductive technologies.[1-9] Ovarian pregnancy accounts for only 1–3% of all ectopic pregnancies and is rarely encountered in association with a concurrent intrauterine gestation.[10]
Diagnosis is often challenging because identification of an intrauterine gestational sac may falsely reassure clinicians and delay recognition of the ectopic component.
Patient Information
A 32-year-old female patient, gravida 7, para 1, abortion 5, living 2 (one twin delivery), presented with 6 weeks of amenorrhea and complaints of lower abdominal pain.
Her obstetric history was significant for one previous full-term normal vaginal delivery of twins. Following this pregnancy, she had undergone five induced abortions. According to the patient, all five abortions were achieved using self-administered medical termination of pregnancy (MTP) pills obtained directly from a pharmacy without prior medical consultation. She did not undergo dilation and evacuation (D&E) or any uterine surgical procedure following any of these abortions.
The most recent medical abortion had been performed approximately three months before the current conception. The patient subsequently conceived spontaneously.
Clinical Presentation
Patient was vitally stable with Pulse: 92 bpm, Blood pressure: 110/70 mmHg, respiratory rate: 18/min, Spo2: 98% on room air. On per vaginal examination uterus as anteverted and bulky in size left fornix was normal while right forniceal fullness and tenderness was present. Initial ultrasonography revealed an ill-defined intrauterine gestational sac and a well-defined gestational sac corresponding to approximately 5 weeks of gestation within the right ovary, suggestive of heterotopic pregnancy. Patient was advised for β-hCG report. Symptomatic treatment was given.
Three days later, the patient presented with bleeding per vaginum associated with persistent lower abdominal pain since 2 days.
Diagnostic Assessment
Repeat ultrasonography (Transvaginal Sonography) demonstrated retained products of conception (RPOC) measuring 2×2 cm within the uterine cavity, while the right ovarian gestational sac persisted. (Figure 1)
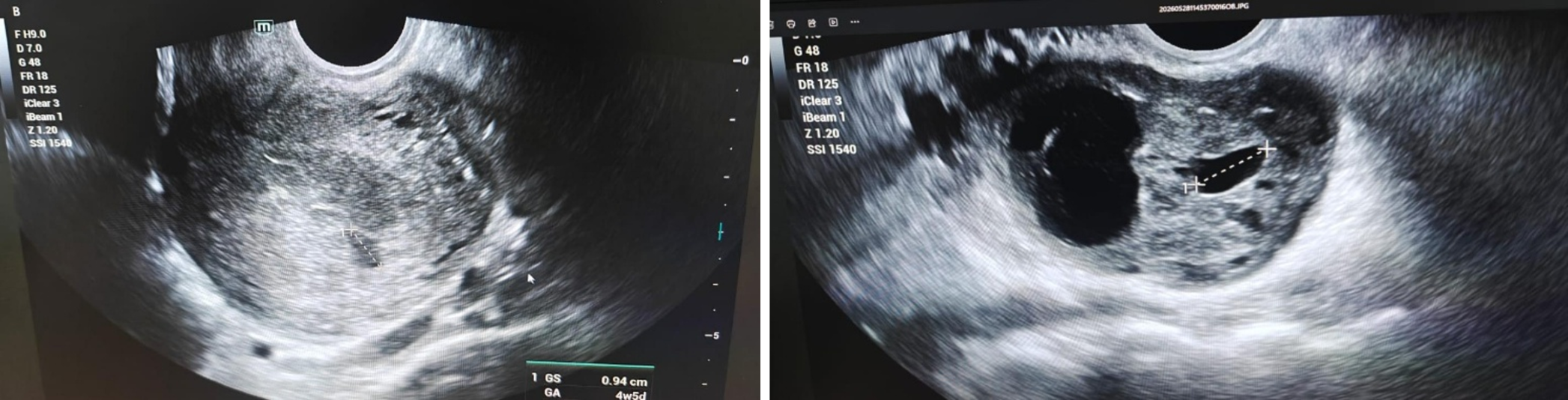
Laboratory investigations revealed: Haemoglobin: 8.4 g/dL and Serum β-hCG: 8,935 IU/L.
Based on clinical and sonographic findings, a diagnosis of spontaneous heterotopic pregnancy consisting of a failed intrauterine pregnancy with persistent right ovarian ectopic gestation was made.
Therapeutic Intervention
Considering the persistent ovarian ectopic pregnancy, pelvic pain, anaemia, and risk of rupture, exploratory laparotomy was performed.
Intraoperatively, a haemorrhagic, highly vascular gestational mass was identified arising from the right ovary. The ipsilateral fallopian tube appeared intact and separated from the ectopic mass. The ovarian swelling demonstrated prominent surface vascularity and dark haemorrhagic areas suggestive of ovarian implantation.
The ectopic gestation was excised successfully. Simultaneously, dilation and evacuation (D&E) was performed for retained products of conception within the uterine cavity.
Operative Findings
The intraoperative findings strongly suggested primary ovarian ectopic pregnancy: Gestational sac occupying the ovary, Haemorrhagic ovarian mass with extensive vascularity, Ipsilateral fallopian tube grossly normal and separate from the lesion and Excised specimen demonstrating gestational sac-like tissue with trophoblastic appearance. (Figure 2)
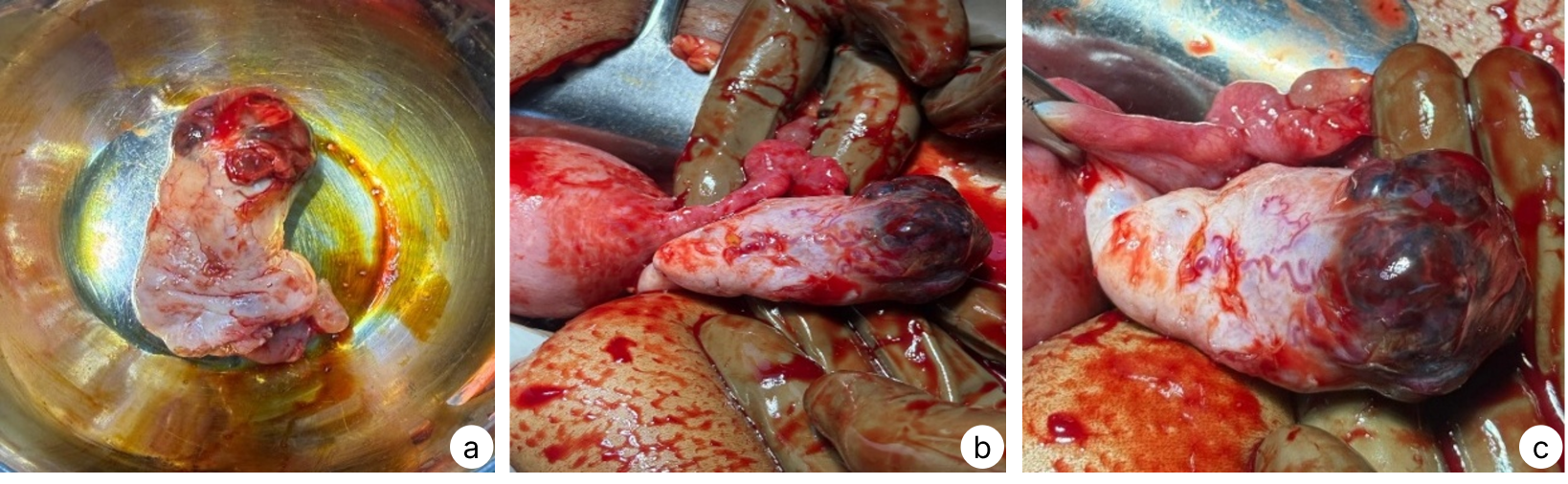
These findings were consistent with ovarian ectopic pregnancy and supported the diagnosis of ovarian heterotopic pregnancy in correlation with preoperative ultrasonographic findings and histopathological finding also confirming the same.
Follow up and Outcome
The postoperative course was uneventful, one-unit packed cell volume (PCV) was given and the patient remained hemodynamically stable throughout recovery.
Discussion
Spontaneous heterotopic pregnancy remains a diagnostic challenge because the presence of an intrauterine gestation may lead clinicians to overlook a coexisting ectopic pregnancy. This case illustrates the importance of careful adnexal evaluation even when an intrauterine gestational sac is visualized.
The uniqueness of this case lies not only in the rarity of ovarian heterotopic pregnancy but also in the clinical course. The intrauterine component subsequently failed and presented as retained products of conception, whereas the ovarian ectopic gestation persisted. Such a presentation can easily be mistaken for an isolated incomplete abortion, potentially delaying diagnosis of the ectopic component.
The patient conceived spontaneously without assisted reproductive techniques and had no history of tubal surgery, pelvic surgery, or uterine instrumentation. Although she had a history of five prior medical abortions, she had never undergone surgical evacuation procedures.
Heterotopic pregnancies can be asymptomatic in about half of the cases. It can be presented with mainly abdominal pain, adnexal swelling that may be associated with bleeding per vaginum, or even hypovolemic shock. Unfortunately, the clinical findings are more frequently presented with tubal rupture.[3–7] While ectopic pregnancy can be early diagnosed during the screening of the serum β-hCG and transvaginal sonography (TVS) in routine prenatal assessment, heterotopic pregnancy diagnosis can be a challenge as it may be delayed in the concurrence of intrauterine pregnancies. This can be due to the differential diagnosis between ectopic pregnancy and other situations that may be associated with normal pregnancy as haemorrhagic corpus luteum or adnexal torsion.[2,6–9] In normal pregnancies, serum β-hCG above 1500–2000 mIU/mL should be associated with ultrasound visualized intrauterine (IU) pregnancy; however, this intrauterine pregnancy will not necessarily exclude the chance of having a heterotopic pregnancy especially in cases receiving conception-assisted techniques.
Ovarian ectopic pregnancy carries a significant risk of rupture because of the highly vascular ovarian tissue. In the present case, surgical management was chosen due to persistent pelvic pain, anaemia, and the continued presence of a viable ectopic gestational mass.
The intraoperative appearance strongly supported the diagnosis of ovarian pregnancy. Histopathological confirmation demonstrating chorionic villi within ovarian tissue would further satisfy the Spiegelberg criteria for primary ovarian pregnancy.
This case highlights a rare presentation of spontaneous heterotopic pregnancy involving a right ovarian ectopic gestation and a concurrent failed intrauterine pregnancy. Persistence of the ovarian ectopic component despite spontaneous abortion of the intrauterine gestation created a potential diagnostic pitfall. Early recognition through serial ultrasonography and prompt surgical management prevented serious maternal morbidity. Clinicians should maintain a high index of suspicion for heterotopic pregnancy in women presenting with abdominal pain and vaginal bleeding, even when an intrauterine gestational sac is identified.
References
- Fernandez H, Gervaise A (2004) Ectopic pregnancies after infertility treatment: modern diagnosis and therapeutic strategy. Hum Reprod Update 10(6):503–513. doi:10.1093/humupd/dmh043
- Callen PW Ultrasonography in obstetrics and gynecology. In: Levine D (ed) Ectopic Pregnancy, 5th edn. Saunders Elsevier, Philadelphia, pp 1020–1047
- Xiao HM, Gong F, Mao ZH, Zhang H, Lu GX (2006) Analysis of 92 ectopic pregnancy patients after in vitro fertilization and embryo transfer. J Cent South Univ 31(4):584–587
- Louis-Sylvestre C, Morice P, Chapron C, Dubuisson JB (1997) The role of laparoscopy in the diagnosis and management of heterotopic pregnancies. Hum Reprod 12(5):1100–1102. doi:10.1093/humrep/12.5.1100
- Jeon HS, Shin HJ, Kim IH, Chung DY (2012) A case of spontaneous heterotopic pregnancy presenting with heart activity of both embryos. Kor J Obstet Gynecol 55(5):339–342. doi:10.5468/KJOG.2012.55.5.339
- Elito NAMD, Montenegro M, Costa Soares RDA, Camano L (2008) Unruptured ectopic pregnancy—diagnosis and treatment. State of art. Revista Brasileira de Ginecologia e Obstetricia 30(3):149–154. doi:10.1590/s0100-72032008000300008
- Dündar Ö, Tütüncü L, Müngen E, Muhcu M, Yergök YZ (2006) Heterotopic pregnancy: tubal ectopic pregnancy and monochorionic monoamniotic twin pregnancy: a case report. Perinatal J 14(2):96–100
- Tamai K, Koyama T, Togashi K (2007) MR features of ectopic pregnancy. Eur Radiol 17(12):3236–3246. doi:10.1007/s00330-007-0751-6
- Li XH, Ouyang Y, Lu GX (2013) Value of transvaginal sonography in diagnosing heterotopic pregnancy after in-vitro fertilization with embryo transfer. Ultrasound Obstet Gynecol 41(5):563–569. doi:10.1002/uog.12341
- Bontis J, Grimbizis G, Tarlatzis BC, Miliaras D, Bili H. Intrafollicular ovarian pregnancy after ovulation induction/intrauterine insemination: pathophysiological aspects and diagnostic problems. Hum Reprod. 1997 Feb;12(2):376-8. doi:10.1093/humrep/12.2.376. PMID: 9070729